




What Is PMOS?
Polyendocrine metabolic ovarian syndrome (PMOS), formerly known as polycystic ovary syndrome (PCOS), is the most common endocrine disorder affecting women of reproductive age worldwide.[^1][^2][^13] PMOS is not primarily about ovarian cysts — it is a complex hormonal condition characterized by higher-than-normal androgen levels, which lead to irregular menstrual periods, abnormal ovulation, and a range of metabolic disturbances.[^1]
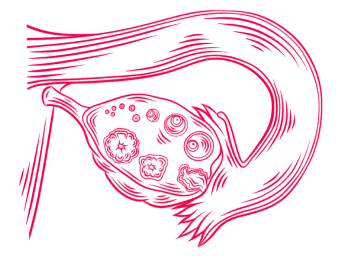
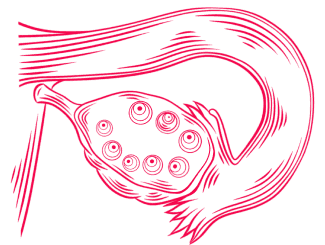
Images: Ovarian Cysts — Normal (Left) VS. Polycystic (Right)
PMOS affects an estimated 10–13% of reproductive-aged women globally.[^1] However, the true prevalence varies between 5% and 26% depending on the diagnostic criteria used and the population studied.[^3] This makes PMOS one of the most significant health concerns for women, yet remarkably, up to 70% of affected women remain undiagnosed.[^1]
The syndrome runs in families and can cause a wide range of symptoms that affect women differently. PMOS is a lifelong condition with metabolic implications that may persist beyond the reproductive years, although diagnostic criteria are primarily defined for reproductive-age women.[^1][^2] Early diagnosis and management are crucial for long-term health.
How Is PMOS Diagnosed? The Rotterdam Criteria
Diagnosing PMOS can be challenging because its symptoms overlap with other conditions. In 2003, a group of 27 international experts met in Rotterdam, Netherlands, to establish standardized diagnostic criteria. These Rotterdam Criteria remain the most widely used and accepted diagnostic framework today.[^4][^5]
According to the Rotterdam Criteria, a diagnosis of PMOS requires at least two of the following three features (after excluding other conditions):[^5]
Criterion | Description |
1. Oligo/anovulation | Irregular or absent menstrual periods due to infrequent or absent ovulation. |
2. Hyperandrogenism | Clinical signs (excess facial/body hair, acne, male-pattern hair loss) or elevated androgen levels on blood tests. |
3. Polycystic ovaries | ≥20 follicles (2–9 mm) in at least one ovary and/or ovarian volume >10 mL on ultrasound.[^2][^5] |
Sources: International Evidence-based Guideline for the Assessment and Management of PMOS 2023[^2] and Christ & Cedars 2023[^5]
Importantly, other conditions that can cause similar symptoms must be ruled out before making a PMOS diagnosis. These include thyroid disorders, hyperprolactinemia, congenital adrenal hyperplasia, and androgen-secreting tumors.[^3][^5]
What Are the Symptoms and Clinical Presentation of PMOS?
PMOS presents with a wide spectrum of symptoms that can vary significantly between women. The condition can start as early as adolescence, but is most commonly detected when women experience difficulty becoming pregnant.[^1][^6]
What Are the Most Common Symptoms?
Menstrual irregularities: This is often the first noticeable sign. Women may experience infrequent periods (oligomenorrhea), absent periods (amenorrhea), or unpredictable cycles. Some women have fewer than nine periods per year.[^1][^6]
Hirsutism: Excess hair growth in male-pattern areas (face, chest, back, and abdomen) affects a large proportion of women with PMOS, with an estimated range from 40–70% depending on ethnicity.[^3][^6] This is caused by elevated androgen levels.
Acne and oily skin: Hormonal acne that persists beyond adolescence, particularly along the jawline and chin, is common in PMOS.[^4]
Hair thinning: Female-pattern hair loss or thinning at the crown of the head can occur due to androgen excess.[^1]
Weight changes: While PMOS occurs in women of all body weights, obesity is common; pooled studies show approximately 61% of women with PMOS have obesity.[^9]
Infertility: PMOS is the most common cause of anovulatory infertility. Many women with PMOS experience ovulatory dysfunction, which can make conception more difficult, though many conceive naturally.[^1][^3]
What Are the Four PMOS Phenotypes?
Because PMOS can present in different combinations of symptoms, the 2012 National Institute of Health (NIH) consensus panel established a phenotypic classification system. Understanding your phenotype helps predict disease severity and guide treatment decisions.[^5][^8]
Phenotype | Features Present | Description | Prevalence |
A | Hyperandrogenism + Ovulatory Dysfunction + Polycystic Ovarian Morphology | Classic PMOS (full-blown) | Approximately 67.7% |
B | Hyperandrogenism + Ovulatory Dysfunction | Non-PCO PMOS | Approximately 11% |
C | Hyperandrogenism + Polycystic Ovarian Morphology | Ovulatory PMOS | Approximately 17.7% |
D | Ovulatory Dysfunction + Polycystic Ovarian Morphology | Non-hyperandrogenic PMOS | Approximately 3.6% |
Source: Sachdeva et al. 2019[^8]
Approximate prevalence; varies by population and criteria used.
Research shows that Phenotype A is generally associated with higher metabolic and cardiovascular risks, including higher BMI, insulin resistance, and deranged lipid profiles. Phenotype D often shows milder metabolic features with better responses to fertility treatment.[^8]
What Hormonal Imbalances Occur in PMOS?
PMOS involves complex hormonal disruptions that affect multiple body systems. Understanding these imbalances helps explain why PMOS causes such varied symptoms.[^7][^10]
What Are the Key Hormonal Changes?
Elevated androgens: Women with PMOS typically have higher levels of testosterone and other male hormones. This causes hirsutism, acne, and disrupts normal ovulation.[^7][^10]
Altered LH/FSH ratio: Many women with PMOS have an elevated luteinizing hormone (LH)/follicle-stimulating hormone (FSH) ratio. High LH stimulates the ovaries to produce more androgens, while relatively low FSH impairs follicle development and ovulation.[^7][^10] Although an elevated LH/FSH ratio may be seen in some women with PMOS, it is not required for diagnosis and is not present in all cases.
Insulin resistance: Insulin resistance is common in PMOS, affecting roughly 50–75% of women, including some who are not overweight.[^3] Elevated insulin stimulates ovarian androgen production and lowers sex hormone-binding globulin (SHBG), further increasing free testosterone levels.[^7][^9]
Low progesterone: Because ovulation is irregular or absent, progesterone levels are often insufficient. This can contribute to irregular periods and increase the risk of endometrial hyperplasia.[^7]
How Does PMOS Affect Fertility and Ovulation?
PMOS is the most common cause of anovulatory infertility and a leading cause of infertility overall.[^1][^3] Understanding how PMOS affects fertility is essential for women planning pregnancy.
How Does PMOS Disrupt Ovulation?
In a normal menstrual cycle, FSH stimulates follicles to grow, and one dominant follicle matures and releases an egg. In PMOS, hormonal imbalances prevent this process:[^7][^11]
Multiple follicles begin developing but fail to mature fully
No dominant follicle emerges, so ovulation does not occur
The underdeveloped follicles remain in the ovaries, creating the characteristic “polycystic” appearance on ultrasound
What Pregnancy Complications Can Occur?
Women with PMOS who become pregnant face higher risks of certain complications:[^2][^11]
Miscarriage (risk may be influenced by associated factors such as obesity and insulin resistance)
Gestational diabetes
Hypertension and preeclampsia
Preterm delivery
Increased likelihood of Caesarean delivery
However, with appropriate monitoring and care, most women with PMOS can have successful pregnancies.[^2]
→ Learn more: Female Infertility
How Is PMOS Diagnosed and Tested?
Diagnosing PMOS involves a thorough evaluation of symptoms, medical history, physical examination, laboratory tests, and imaging. There is no single test that confirms or excludes PMOS.[^3][^5][^6]
What Tests Are Recommended?
Hormone blood tests: These typically include total and free testosterone, sex hormone-binding globulin (SHBG), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and may include dehydroepiandrosterone sulfate (DHEAS) and androstenedione to assess androgen levels.[^5]
Transvaginal ultrasound: To evaluate ovarian morphology and identify polycystic ovarian appearance (≥20 follicles per ovary or ovarian volume >10 mL, per the 2023 international guidelines).[^2][^5][^6]
Metabolic screening: Fasting glucose and insulin, oral glucose tolerance test (OGTT), and lipid panel to assess metabolic status.[^2]
Thyroid function tests: To rule out thyroid disorders that can cause similar symptoms.[^3]
Prolactin levels: To exclude hyperprolactinemia as a cause of irregular periods.[^3]
Images: Testing Procedure — Transvaginal Ultrasound
What Are the Treatment Options for PMOS?
Treatment for PMOS is tailored to individual goals — whether managing symptoms, improving metabolic health, or achieving pregnancy. The 2023 International Evidence-based Guideline provides clear recommendations.[^2]
What Lifestyle Modifications Are Recommended?
Lifestyle intervention is recommended as first-line treatment for all women with PMOS. For women who are above a healthy weight, even modest weight loss of 5–10% can significantly improve symptoms and fertility outcomes. For women at or below a healthy weight, maintaining balanced nutrition and regular physical activity remains beneficial.[^2][^3]
Regular physical activity (both aerobic and resistance training)
Balanced diet focusing on whole foods, fiber, and low glycemic index choices
Weight management tailored to individual needs
Behavioral strategies to support long-term adherence
What Medical Treatments Are Available for Symptoms?
Combined oral contraceptives (COCPs): First-line pharmacological treatment for menstrual irregularities, hirsutism, and acne in women not seeking pregnancy.[^2]
Metformin: An insulin-sensitizing medication that can improve insulin sensitivity and help regulate menstrual cycles. Its effects on weight are generally modest. It is particularly useful in women with insulin resistance.[^2][^4]
Anti-androgens (for example, spironolactone): May be added to COCPs for treating hirsutism and acne when first-line treatments are insufficient.[^2][^4]
What Fertility Treatments Are Available?
For women with PMOS seeking pregnancy, ovulation induction is typically the first step:[^2]
Letrozole: Now recommended as first-line pharmacological treatment for ovulation induction in women with PMOS and anovulatory infertility. Studies show that letrozole achieves higher rates of ovulation, pregnancy, and live birth than clomiphene citrate. It is not used when another infertility factor (for example, tubal blockage or severe male factor) is present without further evaluation.[^2]
Clomiphene citrate: A long-established ovulation induction agent. Can be used alone or combined with metformin. Multiple pregnancy risk requires monitoring.[^2]
Gonadotropins (FSH injections): For women who do not respond to oral medications. Requires careful monitoring due to a higher risk of ovarian hyperstimulation syndrome (OHSS) in PMOS.[^2]
Laparoscopic ovarian surgery (ovarian drilling): May be considered in clomiphene- or letrozole-resistant women as an alternative to gonadotropins.[^2]
In vitro fertilization (IVF): Recommended when other treatments fail or when there are additional infertility factors. Women with PMOS often respond strongly to ovarian stimulation due to higher ovarian reserve, but careful protocols are required to minimize the risk of OHSS. GnRH antagonist protocols with GnRH agonist trigger are preferred.[^2]
What Are the Long-Term Health Considerations?
PMOS is not just a reproductive condition — it has significant implications for long-term health. Women with PMOS face increased risks for several chronic conditions that require ongoing monitoring and management.[^3][^9][^12]
What Are the Metabolic Risks?
Type 2 diabetes: Women with PMOS have a significantly higher risk of developing impaired glucose tolerance and type 2 diabetes. Regular screening with oral glucose tolerance tests is recommended.[^9][^12]
Metabolic syndrome: The risk of metabolic syndrome is more than twofold higher in women with PMOS, even after adjusting for age and BMI.[^9]
Cardiovascular disease: Traditional cardiovascular risk factors are more prevalent in PMOS. Although cardiovascular risk factors are more prevalent, long-term data on cardiovascular events and mortality remain limited and somewhat inconclusive.[^9][^12]
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): Women with PMOS have a 2.2-fold increased risk of MASLD, particularly those with hyperandrogenism.[^9]
What Other Health Concerns Are Associated with PMOS?
Endometrial health: Chronic anovulation and unopposed estrogen exposure increase the risk of endometrial hyperplasia and endometrial cancer. Regular menstrual management is important for protection.[^1][^3]
Obstructive sleep apnea: Women with PMOS have higher rates of sleep apnea, which is associated with increased cardiovascular risk. Risk is particularly increased in women with obesity and significant hyperandrogenism.[^9]
Mental health: Depression and anxiety are significantly more common in women with PMOS. Screening and appropriate treatment should be part of comprehensive care.[^3]
So, What Should You Do Now?
If you suspect you may have PMOS or have already been diagnosed, here are the steps to take control of your health:
Step 1: Recognize the Signs
If you experience irregular periods, excess hair growth, acne, or difficulty conceiving, these may be signs of PMOS. Do not ignore persistent symptoms – early evaluation leads to better outcomes.
Step 2: Get a Thorough Diagnosis
Ask your doctor about the Rotterdam Criteria evaluation, which includes blood hormone tests and a transvaginal ultrasound. A complete metabolic screening is also recommended.
Step 3: Start with Lifestyle Changes
Regardless of your weight, regular physical activity and a balanced diet are the foundation of PMOS management. Even modest improvements can significantly affect symptoms and fertility.
Step 4: Explore Treatment Options
Work with your healthcare provider to determine whether medications, ovulation induction, or assisted reproduction are right for your situation. Letrozole is now the first-line recommendation for ovulation induction in PMOS.
Step 5: Choose the Right Clinic
If fertility treatment is needed, selecting a clinic with experience in PMOS-specific protocols can make a meaningful difference in outcomes.
→ Compare fertility clinics worldwide: MedicalNavigator.com/fertility-clinics
Too Long, Didn’t Read
PMOS affects 10–13% of reproductive-age women and is the leading cause of anovulatory infertility.
Diagnosis requires 2 of 3 Rotterdam criteria: irregular ovulation, elevated androgens, and polycystic ovaries on ultrasound.
Four phenotypes exist (A, B, C, D) – Phenotype A is generally associated with higher metabolic risk, while Phenotype D often shows milder metabolic features.
Insulin resistance affects approximately 50–75% of women with PMOS, driving
many symptoms.
Lifestyle modification is the first-line treatment for all women with PMOS.
Letrozole is now the recommended first-line medication for ovulation induction.
Most women with PMOS can achieve pregnancy with appropriate treatment.
Long-term monitoring for diabetes, cardiovascular risk, and mental health is essential.
References
[^1]: World Health Organization. Polycystic ovary syndrome. Fact sheet. January 2026.
[^2]: Teede H, et al. International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome 2023. Monash University.
[^3]: Shukla A, Rasquin LI, Anastasopoulou C. Polycystic Ovarian Syndrome. [Updated 2025 Jul 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
[^4]: Ghafari A, Maftoohi M, Eslami Samarin M, Barani S, Banimohammad M, Samie R. The last update on polycystic ovary syndrome (PCOS), diagnosis criteria, and novel treatment. Endocrine and Metabolic Science. 2025;18:100228.
[^5]: Christ JP, Cedars MI. Current Guidelines for Diagnosing PCOS. Diagnostics (Basel). 2023;13(6):1113.
[^6]: Lentscher JA, Decherney AH. Clinical Presentation and Diagnosis of Polycystic Ovarian Syndrome. Clin Obstet Gynecol. 2021;64(1):3-11.
[^7]: Phenotypic variations in polycystic ovary syndrome: metabolic risks and emerging biomarkers. 2025.
[^8]: Sachdeva G, Gainder S, Suri V, Sachdeva N, Chopra S. Comparison of the Different PCOS Phenotypes Based on Clinical Metabolic, and Hormonal Profile, and their Response to Clomiphene. Indian J Endocr Metab. 2019;23(3):326-331.
[^9]: Dong J, Rees DA. Polycystic ovary syndrome: pathophysiology and therapeutic opportunities. BMJ Medicine. 2023;2(1):e000548.
[^10]: Yang J, Chen C. Hormonal changes in PCOS. Journal of Endocrinology. 2024;261(1):e230342.
[^11]: McDonnell R, Hart RJ. Pregnancy-related outcomes for women with polycystic ovary syndrome. Women’s Health (London). 2017;13(3):89-97.
[^12]: Allen LA, Shrikrishnapalasuriyar N, Rees DA. Long-term health outcomes in young women with polycystic ovary syndrome: A narrative review. Clin Endocrinol (Oxf). 2022;97:187-198.
[^13]: Teede HJ, Bahri Khomami M, Morman R, et al. Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: a multistep global consensus process. Lancet. 2026 May 12;S0140-6736(26)00717-8. doi: 10.1016/S0140-6736(26)00717-8.
This guide is for informational purposes only. Always consult qualified healthcare providers for personalized recommendations. For full details, read our Medical Disclaimer.

Author of the article
Date of publication


