




What Is Ovulation?
Ovulation is the process by which a mature egg is released from the ovary, making it available for fertilisation.[^2][^3] This process is controlled by a complex hormonal communication system between the brain and the ovaries, known as the hypothalamic–pituitary–ovarian (HPO) axis.[^3] When this system functions normally, an egg is released in a relatively predictable and cyclical fashion.[^2]
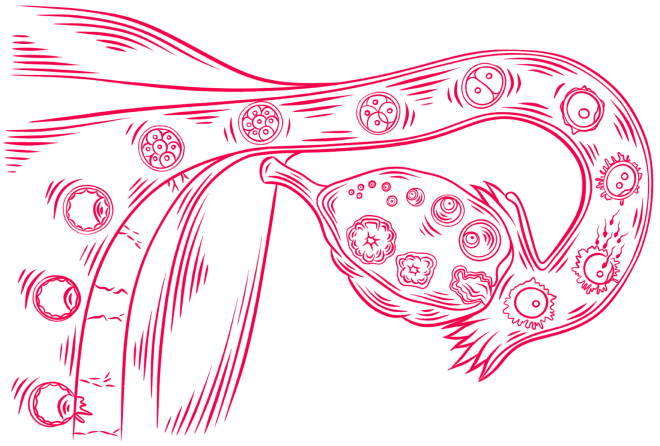
Image: Ovulation & Fertilization — Egg Release and Embryo Development in the Fallopian Tube
What Are Ovulatory Disorders?
Ovulatory disorders occur when the full ovulation process is disrupted, or it doesn’t happen regularly.[^1] They can affect bone density, metabolic health, and cardiovascular risk over time, and they are a common cause of infertility.[^1][^2] In simple terms, your body either isn’t releasing eggs at all or it’s not releasing them on a predictable schedule.
The International Federation of Gynaecology and Obstetrics (FIGO) has developed a comprehensive classification system to help doctors understand exactly where, along the ovulatory process, things aren’t working as they should.[^2][^3] This system recognises that ovulatory disorders exist on a spectrum — from occasional missed ovulations to chronic ovulatory failure.

Image: The HPO Axis — The Brain, Pituitary Gland, and Ovary Working Together to Control Ovulation
Why Do They Matter Beyond Fertility?
Many people think ovulation disorders only matter if you’re trying to get pregnant, but this isn’t true. Irregular ovulation can affect bone, metabolic, and heart health over time.[^1] These disorders profoundly affect quality of life, leading to disturbances in menstrual function and a range of hormone-related symptoms.[^3]
Research has found that having persistently irregular menstrual cycles is linked with heightened risk for cardiometabolic conditions.[^1] This highlights how impactful ovulation disorders can be on overall health — not just reproductive health.
What Are the Four Types of Ovulatory Disorders?
The FIGO classification system divides ovulatory disorders into four main types, remembered by the acronym HyPO-P (Hypothalamic, Pituitary, Ovarian, PCOS).[^2][^3] Each type is based on where the problem originates in your body.
Type | Location | What Happens |
Type I | Hypothalamus | The brain’s command centre for hormone signals isn’t working properly. |
Type II | Pituitary | Problems with how the brain and ovaries communicate. |
Type III | Ovarian | The ovaries don’t respond to signals (including Primary Ovarian Insufficiency, or POI). |
Type IV | Polycystic Ovary Syndrome (PCOS) | A complex hormonal imbalance affects the whole body. |
Source: FIGO Ovulatory Disorders Classification System (2022)[^2] and Balen et al.
Type I — Hypothalamic Disorders
These disorders involve dysfunction of the hypothalamus, a region of the brain that acts as a central command centre for ovarian hormones.[^1][^3] Common examples include women who stop ovulating due to significant psychological stress, athletes who don’t fuel themselves with enough energy, or those with eating disorders.

Image: The Pituitary Gland (Hypophysis) — Brain's Hormonal Control Centre
Functional hypothalamic amenorrhoea (FHA) accounts for about 20–35% of cases of secondary amenorrhoea and up to 48% of cases in adolescent girls.[^3][^6] There is a tight link between activation of the stress response system (hypothalamic–pituitary–adrenal, or HPA, axis) and reduced gonadotropin-releasing hormone (GnRH) secretion in those with FHA.[^3]
Type II — Pituitary Disorders
The pituitary gland is a small gland located at the base of the brain that produces hormones controlling many body functions, including reproduction.[^3] These disorders involve issues with how the pituitary gland communicates with the ovaries.
Hormone levels may be abnormal, or sometimes inappropriately normal relative to the clinical situation, leading to disrupted ovulation.[^1][^3] When the brain is under perceived stress, it can put reproductive processes on hold as it prepares to save energy or focus on survival.[^1]
Pituitary tumours (adenomas) can interfere with normal hormonal function. A common example is hyperprolactinaemia, a condition characterised by elevated prolactin levels, which can lead to galactorrhoea (unexpected milk production), amenorrhoea (absence of menstrual periods), and infertility.[^3] A prolactinoma should be considered after excluding other common causes of hyperprolactinaemia, including pregnancy, hypothyroidism, and medication-induced prolactin elevation.[^3]
Type III — Ovarian Disorders
These disorders happen when there are issues with the ovaries themselves. It’s like they have ‘Do Not Disturb’ turned on — no matter how many times the brain tries to call, the ovaries never ‘answer’ to ovulate (to release an egg from the ovary).[^1]
Image: The Ovary — Where Eggs Mature and Are Released During Ovulation
The main condition in this category is Primary Ovarian Insufficiency (POI), previously called premature ovarian failure. POI is defined as the development of hypergonadotropic hypogonadism before the age of 40, with at least 4 months of oligo/amenorrhoea or menstrual irregularity and elevated follicle-stimulating hormone (FSH) levels on two occasions at least 4 weeks apart.[^3][^7] The exact incidence is unknown as many cases go undiagnosed, but studies suggest it affects about 1:1,000 women by age 30 and 1:100 by age 40.[^3][^7]
Causes of POI include genetic abnormalities, exposure to chemotherapy that is toxic to the ovaries, pelvic radiation therapy, and, less commonly, several autoimmune disorders that affect ovarian tissue.[^1][^7]
Type IV — Polycystic Ovary Syndrome (PCOS)
PCOS is given its own category because it’s a complex disorder affecting the whole body that cannot be confined to a single anatomic origin.[^2][^3] It is the most common ovulatory disorder, affecting 6–12% of reproductive-age women, yet it remains significantly underdiagnosed.[^1][^5]

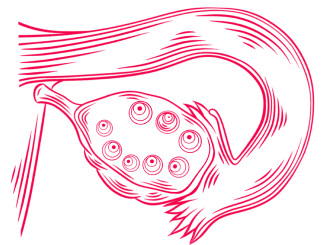
Images: Ovarian Cysts — Normal (Left) VS. Polycystic (Right)
Although PCOS affects the ovaries, it is driven by complex hormonal and metabolic interactions involving the ovaries, brain, and endocrine system.[^1][^3] PCOS has no single known cause. Instead, it is thought to result from a combination of genetic, environmental, and metabolic factors.[^1][^3][^5]
What Causes Ovulatory Disorders?
Ovulatory dysfunction is caused by disorders of the hypothalamic–pituitary–ovarian (HPO) axis, which may be permanent, temporary, or episodic.[^3] While some causes are genetic or related to structural problems, many common but often underdiscussed influences include:
Psychological stress — can activate the HPA axis and reduce GnRH secretion[^3][^6]
Eating disorders — anorexia nervosa accounts for 15–35% of secondary amenorrhoea cases[^3]
Low body weight — adequate body fat is necessary to maintain ovulatory cycles, although the exact threshold varies between individuals[^3]
Excessive exercise — menstrual disturbance affects 10–20% of athletes undergoing intensive training[^3]
Thyroid dysfunction — can lead to anovulation via direct and indirect actions on the HPO axis[^3][^11][^12]
Obesity — metabolic factors can disrupt hormonal signalling[^3]
Sometimes, the reasons are unknown. When this happens, doctors call the cause “idiopathic” — it simply means that the underlying cause has not yet been identified.[^1]
What Are the Symptoms of Ovulatory Disorders?
Most ovulatory disorders are suggested by abnormal menstrual bleeding patterns, ranging from complete absence (amenorrhoea) to infrequent or irregular onset of menstrual bleeding.[^2][^3]
Parameter | Normal | Concern |
Cycle length | 24–38 days | <24 or >38 days |
Cycle regularity (ages 26–41) | ±7 days variation | >7 days variation |
Secondary amenorrhoea | N/A | ≥3 months without menstruation (if cycles were previously regular) or ≥6 months (if cycles were irregular) |
Source: FIGO AUB System 1 (Munro et al., 2018)[^2] and Balen et al. (2024)[^3]; Klein et al. (2019)[^9]
Important:
Women with regular cycles may still occasionally not ovulate. The frequency of single-cycle anovulation in women with normal regular cycles ranges approximately from 3.7–26.7%.[^2][^3] This means you could have seemingly normal periods but still have an ovulatory disorder.
How Are Ovulatory Disorders Diagnosed?
According to experts, the first step is visiting your doctor so you can get the right tests.[^1] Your clinician will perform a targeted physical examination and ask questions about your family and medical history, health concerns, and lifestyle.[^1][^8]
Key Diagnostic Tests
Test | What It Checks |
FSH and LH levels | Pituitary function and ovarian reserve. |
AMH (Anti-Müllerian Hormone) | Reflects ovarian follicle pool (ovarian reserve), but does not confirm whether ovulation is occurring. Not cycle dependent. |
Prolactin | Pituitary tumours, medication effects. |
Thyroid function (TSH) | Thyroid disorders affecting ovulation. |
Androgens (testosterone) | PCOS and other hormonal imbalances. |
Pelvic ultrasound | Ovarian structure, follicle count, PCOS signs. |
Source: Balen et al. (2024)[^3] and Klein et al. (2019)[^9]
Image: Female Diagnosis — Pelvic Ultrasound for Uterine and Ovarian Assessment
The clinician evaluates all information from exams, tests, and discussions to make a diagnosis, then walks you through what you need to know.[^1]
How Do Ovulatory Disorders Affect Fertility?
Ovulatory disorders are a common cause of infertility.[^2][^12] Chronic anovulation, in particular, contributes significantly because without ovulation, no egg is released for fertilisation.[^2][^3] However, the good news is that many ovulatory disorders are among the most treatable causes of female infertility.
Women who present with infertility may also report menstrual symptoms suggestive of an ovulatory disorder, such as irregular or absent periods.[^2] Thyroid dysfunction, in particular, can lead to anovulation and reduced fertility through both direct effects on the ovaries and indirect effects on the hypothalamic–pituitary–ovarian (HPO) axis.[^3][^11]
→ Learn more: Female Infertility
What Are the Treatment Options?
Treatment depends on the underlying cause and your goals (managing symptoms versus achieving pregnancy). The FIGO classification helps doctors target treatment precisely.[^3]
Lifestyle Modifications
For functional hypothalamic amenorrhoea, cognitive behavioural therapy has been shown to help the recovery of ovarian activity.[^3] Achieving a healthy lifestyle and body weight is the essential first step, particularly for those with PCOS.[^3][^5]
Medical Treatment
Thyroid disorders: Levothyroxine replacement restores euthyroid status and normal ovulation.[^3][^13]
Hyperprolactinaemia: Dopamine agonists (cabergoline, bromocriptine) are first-line treatment.[^3]
PCOS: Letrozole is first-line for ovulation induction, followed by gonadotropin therapy if needed.[^3][^5]
POI: Hormone replacement therapy and oocyte donation for those desiring fertility.[^3][^7]
Assisted Reproductive Technology
If pregnancy does not occur despite ovulation and appropriate treatment, assisted reproductive technologies such as IVF may be considered based on individual factors.[^4] The National Institute for Health and Care Excellence (NICE) guidelines provide comprehensive recommendations for fertility treatment in women with ovulation disorders.[^4]
→ Learn more: Assisted Reproductive Technology
What Is It Like Living with an Ovulatory Disorder?
Ovulatory disorders can be truly impactful on day-to-day life, and they aren’t in your head.[^1] Research shows that these conditions significantly affect quality of life across multiple dimensions.
Several endocrine disorders that disrupt ovulation are associated with reduced quality of life.[^14] Women with primary ovarian insufficiency experience decreased health-related quality of life compared to women with normal ovarian function.[^15] Additionally, patients with hypothalamic–pituitary–adrenal axis dysregulations show significantly altered quality of life, with more than half experiencing psychological distress requiring attention.[^16]
If you’re struggling with an ovulation disorder, you’re not alone. Your quality of life matters.[^1] Monitoring your menstrual cycle patterns can provide valuable insights to both you and your healthcare team.
So, What Should You Do Now?
If you suspect you may have an ovulatory disorder, here are the steps you can take:
Step 1: Track Your Cycles
Note the length, regularity, and any unusual symptoms. This information is valuable for your doctor.
Step 2: See Your Doctor
If your cycles are consistently irregular, absent, or if you’re having difficulty conceiving, schedule an appointment with your healthcare provider.
Step 3: Be Honest About Lifestyle Factors
Stress, diet, exercise, and weight all matter. Share these openly with your clinician.
Step 4: Ask Questions
Understanding your diagnosis using the FIGO HyPO-P classification can inform your treatment options.
Step 5: Choose the Right Clinic
Finding a clinic with the right expertise can make all the difference in your treatment journey.
→ Compare fertility clinics worldwide: MedicalNavigator.com/fertility-clinics
Too Long, Didn’t Read
Ovulatory disorders occur when ovulation is disrupted or irregular — they affect whole-body health, not just fertility.
The FIGO HyPO-P classification divides them into four types: Hypothalamic, Pituitary, Ovarian, and PCOS.
PCOS is the most common type, affecting 6–12% of reproductive-age women, yet remains underdiagnosed.
Common causes include stress, eating disorders, low body weight, excessive exercise, and thyroid problems.
Normal cycle length is 24–38 days — consistently longer, shorter, or irregular cycles warrant investigation.
Many ovulatory disorders are highly treatable — early diagnosis and appropriate treatment can restore ovulation.
References
[^1]: Huffman E. Understanding Ovulation Disorders: Types, Causes, and New Research. Harvard T.H. Chan School of Public Health, Mahalingaiah Lab. September 2025.
[^2]: Munro MG, Balen AH, Cho S, et al. The FIGO Ovulatory Disorders Classification System. Human Reproduction. 2022;37(10):2446-2464.
[^3]: Balen AH, Tamblyn J, Skorupskaite K, Munro MG. A comprehensive review of the new FIGO classification of ovulatory disorders. Human Reproduction Update. 2024;30(3):355-382.
[^4]: National Institute for Health and Care Excellence. Fertility problems: assessment and treatment. NICE guideline CG156. 2013 (updated 2017).
[^5]: Teede HJ, Tay CT, Laven JJE, et al. Recommendations From the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2023;108(10):2447-2469.
[^6]: Morrison AE, Fleming S, Levy MJ. A review of the pathophysiology of functional hypothalamic amenorrhoea in women subject to psychological stress, disordered eating, excessive exercise or a combination of these factors. Clin Endocrinol (Oxf). 2021;95(2):229-238.
[^7]: Sopiarz N, Sparzak PB. Primary Ovarian Insufficiency. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
[^8]: Sanchez Jimenez JG, De Jesus O. Hypothalamic Dysfunction. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
[^9]: Klein DA, Paradise SL, Reeder RM. Amenorrhea: A Systematic Approach to Diagnosis and Management. Am Fam Physician. 2019;100(1):39-48.
[^10]: Rugge B, Balshem H, Sehgal R, et al. Screening and Treatment of Subclinical Hypothyroidism or Hyperthyroidism. Comparative Effectiveness Reviews, No. 24. Rockville (MD): AHRQ; 2011.
[^11]: Concepción-Zavaleta MJ, Coronado-Arroyo JC, Quiroz-Aldave JE, et al. Thyroid dysfunction and female infertility. A comprehensive review. Diabetes Metab Syndr. 2023;17(11):102876.
[^12]: Mikhael S, Punjala-Patel A, Gavrilova-Jordan L. Hypothalamic-Pituitary-Ovarian Axis Disorders Impacting Female Fertility. Biomedicines. 2019;7(1):5.
[^13]: National Institute for Health and Care Excellence. Thyroid disease: assessment and management. NICE guideline NG145. 2023.
[^14]: Molewijk E, Fliers E, Dreijerink K, van Dooren A, Heerdink R. Quality of life, daily functioning, and symptoms in hypothyroid patients on thyroid replacement therapy: A Dutch survey. J Clin Transl Endocrinol. 2024;35:100330.
[^15]: McDonald IR, Welt CK, Dwyer AA. Health-related quality of life in women with primary ovarian insufficiency: a scoping review of the literature and implications for targeted interventions. Hum Reprod. 2022;37(12):2817-2830.
[^16]: De Bucy C, Guignat L, Niati T, Bertherat J, Coste J. Health-related quality of life of patients with hypothalamic-pituitary-adrenal axis dysregulations: a cohort study. Eur J Endocrinol. 2017;177(1):1-8.
[^17]: Singh S, Haq N, Sandhu S. Thyroid Disease and Pregnancy. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
This guide is for informational purposes only. Always consult qualified healthcare providers for personalized recommendations. For full details, read our Medical Disclaimer.

Author of the article
Date of publication


