




What Is Tubal Factor Infertility?
Tubal factor infertility occurs when one or both fallopian tubes are blocked, damaged, or otherwise unable to function properly.[^1][^3] The fallopian tubes play a crucial role in reproduction: they capture the released egg from the ovary, provide the environment where fertilization takes place, and transport the early embryo toward the uterus for implantation.[^4]
When these tubes are compromised, the egg and sperm cannot meet, or the fertilized egg cannot reach the uterus. Tubal disorders such as blocked fallopian tubes are often caused by untreated sexually transmitted infections (STIs), complications of unsafe abortion, postpartum sepsis, or abdominal and pelvic surgery.[^1]
Female factors account for approximately 30–40% of infertility cases overall, and tubal factors represent about 20–30% of female infertility.[^3][^4]
→ Learn more: Female Infertility
What Are the Types of Tubal Pathology?
Several conditions can affect the fallopian tubes. Understanding the specific type helps guide treatment decisions.[^4][^5]
What Is Hydrosalpinx?
Hydrosalpinx is a relatively common condition where secretions accumulate in a blocked fallopian tube, preventing them from escaping through the fimbriated end into the peritoneal cavity.[^4] Pelvic inflammatory disease (PID) is the most common cause of distal tubal occlusion and hydrosalpinx, with other less frequent causes including endometriosis, paratubal adhesions from previous surgeries, tubal tumors, and tubal ectopic pregnancies.[^4][^5]
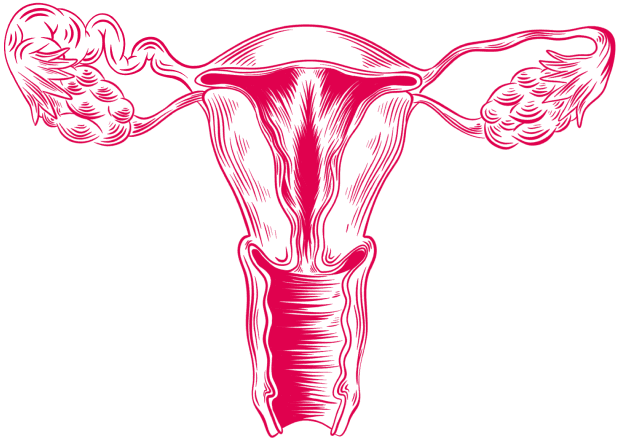
Image: Tubal Factor Infertility — Blocked Fallopian Tube (Hydrosalpinx)
The presence of hydrosalpinx is associated with lower total fertility rates and increased risk of ectopic pregnancy and miscarriage, possibly due to embryotoxic components in the hydrosalpinx fluid.[^4][^8] Evidence strongly supports salpingectomy or proximal occlusion prior to in vitro fertilization (IVF) to improve pregnancy rates, while natural conception rates after reconstructive surgery depend on the severity of tubal damage.[^4][^8]
How Does Pelvic Inflammatory Disease (PID) Affect Fertility?
PID, in the majority of cases, is linked to sexually transmitted infections such as Chlamydia trachomatis and Neisseria gonorrhoeae.[^4][^6] The infection often ascends from the lower genital tract to the uterus, fallopian tubes, and ovaries. PID can result in scarring, adhesions, and partial or total occlusion of the fallopian tubes.[^4]
Infertility risk rises with recurrent PID episodes and the severity of infection. In classic studies, the incidence of infertility was 10–12% after one episode, 23–35% after two episodes, and 54–75% after three episodes.[^3] PID is considered the main cause of tubal adhesions and acquired abnormalities, with early treatment being the key factor influencing the disease’s outcomes and progression.[^4][^5]
How Does Tubal Endometriosis Affect Fertility?
Tubal endometriosis is characterized by the presence of ectopic endometrial implants on the fallopian tubes.[^4][^9] Microscopic tubal endometriosis is more common in individuals with endometriosis than macroscopic disease.[^4] In rare cases, bleeding from these implants may lead to hematosalpinx.[^4]
Tubal endometriosis is associated with advanced stages of the disease and is strongly linked to infertility.[^4][^9] Besides causing scarring on the tubes, endometriosis also leads to inflammation in the pelvis, with elevated reactive oxygen species (ROS) — harmful molecules that increase inflammation and cellular stress — in the tubal fluid, negatively impacting sperm, oocyte, and embryo viability.[^4][^9]
What Is Salpingitis Isthmica Nodosa (SIN)?
The isthmic portion of the fallopian tube can develop nodular swelling of up to a few centimeters in diameter. While the exact cause remains unknown, it is likely due to an acquired process, with studies suggesting a link between SIN and past Chlamydia trachomatis infection.[^4] Its prevalence in healthy, fertile women ranges from 0.6% to 11%; prevalence varies depending on diagnostic criteria and population studied.[^4] SIN is significantly more likely to occur in cases of ectopic pregnancy and infertility.[^4]
A prospective cohort study found that approximately 10.8% of women with laparoscopically confirmed acute salpingitis who attempted pregnancy were infertile due to post-inflammatory tubal blockage.[^4]
How Does Ectopic Pregnancy Relate to Tubal Infertility?
Ectopic pregnancy occurs in about 1–2% of pregnancies, with over 98% implanting in the fallopian tubes.[^4] Risk factors are associated with previous fallopian tube injury, including prior abdominal or pelvic surgery and PID.[^4]
After an ectopic pregnancy, the chance of having an intrauterine pregnancy is approximately 52%, and the risk of a recurrent ectopic pregnancy is about 12.6%.[^4][^15]
What Are the Causes and Risk Factors?
Understanding what causes tubal damage helps with both prevention and treatment planning.[^4][^5][^6]
Category | Risk Factors |
Infectious Agents | Chlamydia trachomatis, Neisseria gonorrhoeae (gonorrhea)[^4][^6][^7] |
Infectious Syndromes | Pelvic inflammatory disease (PID), postpartum infections, post-abortion infections[^4][^5][^6] |
Surgical History | Previous pelvic or abdominal surgery, tubal ligation, appendectomy[^1][^4][^5] |
Endometriosis | Pelvic adhesions, tubal scarring, inflammatory damage[^4][^9] |
Previous Ectopic | History of ectopic pregnancy increases recurrence risk to about 12.6%[^4][^15] |
Source: Based on WHO,[^1] El-Kharoubi (2023),[^4] Hauser (2025),[^5] Tao (2018),[^6] and Trindade (2022)[^15]
What Is the Chlamydia Connection?
Chlamydia trachomatis infection plays a significant role in tubal factor infertility. Meta-analyses show that positivity for Chlamydia-specific IgG antibodies is significantly associated with increased risk of developing tubal factor infertility and ectopic pregnancy.[^7]
In some clinical settings, Chlamydia-specific IgG antibody testing has been introduced as a screening tool for identifying the risk of tubal factor infertility in the infertility work-up, to select high-risk patients for laparoscopic tubal evaluation.[^7]
What Are the Symptoms and Clinical Presentation?
One of the challenging aspects of tubal factor infertility is that it often presents with no obvious symptoms.[^2][^4] Many women only discover they have tubal problems when they experience difficulty conceiving.
When symptoms do occur, they may include:
Pelvic pain (especially with hydrosalpinx or endometriosis)[^4][^9]
Abnormal vaginal discharge[^5]
Painful periods (dysmenorrhea)[^9]
History of pelvic inflammatory disease[^4][^5]
Previous ectopic pregnancy[^4][^15]
How Is Tubal Factor Infertility Diagnosed?
Accurate diagnosis of tubal pathology is essential for determining the best treatment approach. Several methods are available.[^2][^3][^11][^12][^13]
What Is Hysterosalpingography (HSG)?
Hysterosalpingography (HSG) is commonly used as an initial test to assess tubal patency.[^4][^11] It involves injecting contrast dye through the cervix and taking X-ray images to visualize the uterine cavity and fallopian tubes. If tubes are open, dye spills into the pelvic cavity.
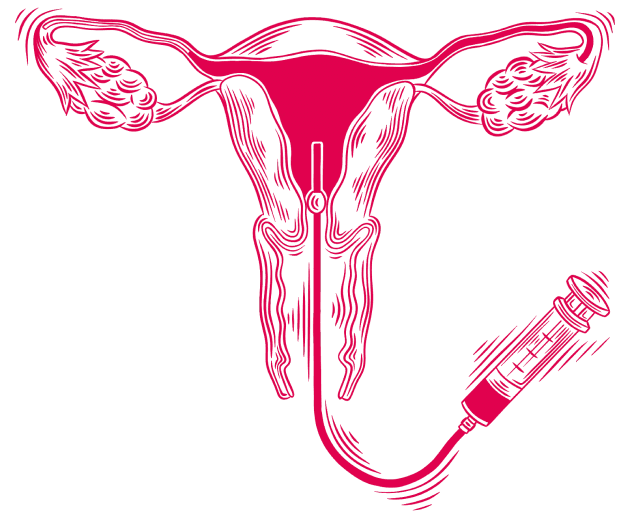
Image: Uterus — Hysterosalpingography (HSG)
What Is Hysterosalpingo-Contrast Sonography (HyCoSy)?
HyCoSy uses ultrasound with contrast media to assess tubal patency. Studies show that air/saline HyCoSy has a high negative predictive value (around 95%), meaning that if the test shows the tubes are open, they are very likely to be truly open.[^12] This procedure can be performed as a screening examination to avoid the use of more expensive contrast media.
What Is Laparoscopy with Chromopertubation?
Laparoscopy is considered the gold standard for evaluating tubal factors, though it is not a screening test due to its invasive nature.[^12][^13] It provides direct visualization of the tubes and pelvis, allowing assessment of adhesions, endometriosis, and tubal damage while offering simultaneous treatment opportunities.
How Does Tubal Factor Infertility Affect Fertility and Reproduction?
Tubal factor infertility has significant implications for natural conception and assisted reproductive technology outcomes.[^3][^4][^8][^14][^15]
What Is the Impact on Natural Conception?
When both tubes are completely blocked, natural conception is extremely unlikely without medical intervention.[^3] Even partial blockage or damage significantly reduces the chances of the egg and sperm meeting.
For women with hydrosalpinx, the natural pregnancy rate within two years following neosalpingostomy (a surgical procedure that creates a new opening in a blocked fallopian tube) was 50% for mild, 17% for moderate, and 16% for severe cases.[^4] Success depends on patient age and the degree of tubal damage.
How Does Hydrosalpinx Affect IVF Outcomes?
The presence of hydrosalpinx reduces the overall success rate of IVF.[^4][^8] Research indicates that hydrosalpinges adversely affect markers of endometrial receptivity, potentially explaining poorer IVF outcomes.[^3] The success rate of IVF-assisted pregnancy for patients with hydrosalpinx was found to be approximately 30–50% lower than for those without hydrosalpinx.[^8]
Salpingectomy, a surgical procedure in which the affected fallopian tube is removed, has been associated with higher rates of IVF live births, clinical pregnancies, and implantations compared to other hydrosalpinx treatments.[^4][^8]
What Is the Ectopic Pregnancy Risk After Assisted Reproduction?
Tubal factor infertility is a significant risk factor for ectopic pregnancy after IVF. The overall rate of ectopic pregnancy following assisted reproductive technology (ART) is approximately 2–3%.[^15] In one study population undergoing ART, tubal factor infertility was associated with a higher relative risk of ectopic pregnancy compared to other infertility causes.[^15] In high-risk patients, a single blastocyst transfer seems to be a reasonable approach to decrease ectopic pregnancy risk.[^15]
What Are the Treatment Options?
Modern medicine offers multiple effective approaches for tubal factor infertility. The best option depends on the type and severity of tubal damage, age, and other fertility factors.[^3][^4][^8][^11]
What Surgical Options Are Available?
Salpingectomy (Tube Removal)
For women with hydrosalpinx planning IVF, salpingectomy before treatment improves outcomes. Studies show this approach has been associated with higher rates of IVF live births compared to other treatments.[^4][^8]
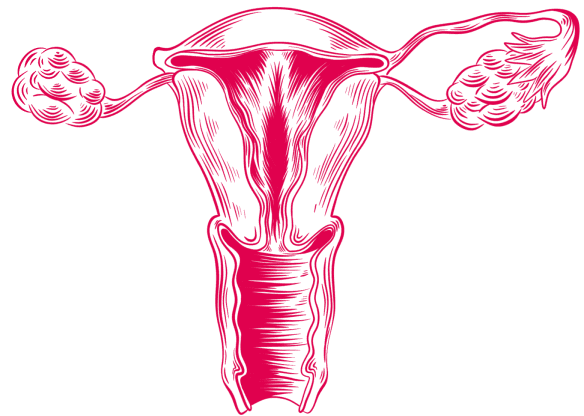
Image: Uterus — Salpingectomy (Tube Removal)
Salpingostomy and Fimbrioplasty
These procedures create a new opening in a blocked tube or address the fimbriated end of the tube. They are suitable for small, thin-walled hydrosalpinx with healthy mucosa.[^4][^11]
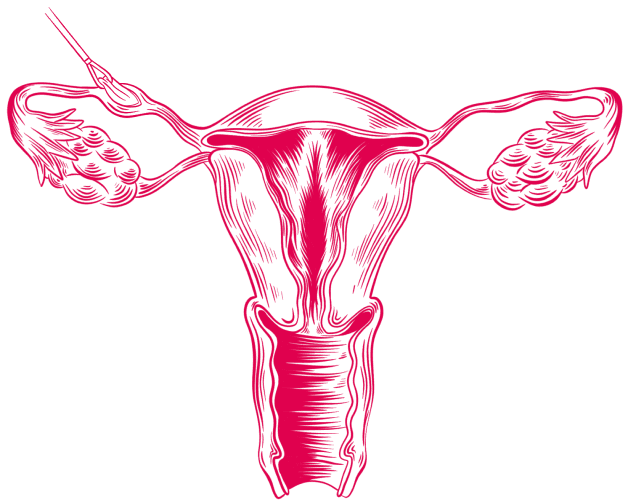
Image: Uterus — Salpingostomy (New Opening in a Blocked Tube)
Proximal Tubal Occlusion
Proximal tubal occlusion involves surgically blocking the fallopian tube near the uterine end to prevent hydrosalpingeal fluid from entering the uterine cavity. Proximal tubal occlusion and salpingectomy result in similar improvement in IVF outcomes in patients with hydrosalpinx.[^3] Research recommends oocyte retrieval should be performed within 7 months after tubal occlusion for hydrosalpinx treatment, with an optimal time of 3 months.[^8]
Tubal Reversal (Tubal Anastomosis)
Tubal anastomosis is a microsurgical procedure that reconnects previously ligated fallopian tubes in women who desire pregnancy after prior sterilization. Laparoscopic tubal anastomosis has shown good fertility outcomes, though success depends on the type of sterilization and the amount of remaining healthy tube.[^3]
Image: Uterus — Tubal Reversal
How Does In Vitro Fertilization (IVF) Help?
IVF effectively bypasses the fallopian tubes entirely. Developed in the late 1970s and in clinical use for over four decades, it provides a solution for individuals facing infertility due to tubal problems.[^4]
With assisted reproductive technology and combined hydrosalpinx treatment, a 61% cumulative pregnancy rate has been reported.[^4] This figure refers to cumulative rates across multiple cycles and may vary significantly by age, clinic, and individual circumstances.
Treatment Comparison
Treatment | Best For | Considerations |
Salpingectomy | Hydrosalpinx before IVF | Improves IVF success rates[^4][^8] |
Salpingostomy | Mild tubal disease | May preserve natural conception[^4][^11] |
Tubal Reversal | Post-sterilization | Success depends on tube health[^3] |
IVF | Severe tubal damage, bilateral blockage | Bypasses tubes entirely[^4] |
Source: Based on ASRM recommendations and published studies[^3][^4][^8][^11]
What Does Living with the Diagnosis Look Like?
A diagnosis of tubal factor infertility can be emotionally challenging. Infertility has significant negative social impacts, and women frequently experience emotional stress, depression, anxiety, and low self-esteem.[^1][^16][^17]
How Can Tubal Factor Infertility Be Prevented?
Some causes of tubal factor infertility are preventable.[^1][^5][^6]
Practice safe sex, including consistent condom use and regular STI testing, to prevent infections such as Chlamydia and gonorrhea[^1][^6]
Seek early treatment for any pelvic infections[^5]
Get regular STI screening, especially before planning pregnancy[^6]
Discuss fertility implications before elective pelvic surgeries[^1]
Where Can You Find Emotional Support?
The psychological impact of infertility is significant. Studies show that infertility may cause emotional distress comparable to that seen in other chronic medical conditions.[^16][^17] Consider seeking support from mental health professionals specializing in fertility, support groups for individuals experiencing infertility, and open communication with your healthcare team about emotional concerns.
So, What Should You Do Now?
If you suspect tubal factor infertility or have been diagnosed, here are the steps you can take to move forward:
Step 1: Get a Proper Diagnosis
Talk to your doctor about having a tubal patency test, such as HSG or HyCoSy. If results are inconclusive, ask about laparoscopy for a definitive assessment.
Step 2: Understand Your Specific Condition
Not all tubal problems are the same. Ask your specialist whether your diagnosis is hydrosalpinx, PID-related damage, endometriosis, or SIN, as each may require a different treatment approach.
Step 3: Explore Your Treatment Options
Depending on the severity, your options may range from surgical correction to IVF. If you have hydrosalpinx, treating it before IVF significantly improves your chances.
Step 4: Address STI Prevention
If infection was a contributing factor, ensure both partners are tested and treated. Practice safe sex, including consistent condom use and regular STI screening, to prevent further damage.
Step 5: Seek Emotional Support
Infertility can take a toll on mental health. Consider speaking with a mental health professional who specializes in fertility-related concerns, and connect with support groups.
Step 6: Choose the Right Fertility Clinic
Success rates vary between clinics. Research and compare fertility clinics that have experience treating tubal factor infertility and offer the full range of treatment options.
→ Compare fertility clinics worldwide: MedicalNavigator.com/fertility-clinics
Too Long, Didn’t Read
Tubal factor accounts for approximately 20–30% of female infertility—blocked or damaged tubes prevent the egg and sperm from meeting.
Main causes include STIs (especially Chlamydia), PID, endometriosis, previous surgery, and ectopic pregnancy.
The condition often has no symptoms—diagnosis is made through HSG, HyCoSy, or laparoscopy.
Hydrosalpinx reduces IVF success by approximately 30–50%, and treatment before IVF significantly improves outcomes.
Treatment options include surgery (salpingectomy, tubal occlusion) or IVF (which bypasses tubes entirely).
Prevention is key: safe sex with consistent condom use, early STI treatment, and regular screening.
References
[^1]: World Health Organization. Infertility Fact Sheet. November 2023.
[^2]: Adebisi OY, Singh M, Tobler KJ. Female Infertility. [Updated 2025 Nov 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
[^3]: Dun EC, Nezhat CH. Tubal factor infertility: diagnosis and management in the era of assisted reproductive technology. Obstet Gynecol Clin North Am. 2012;39(4):551-566.
[^4]: El-Kharoubi AF. Tubal Pathologies and Fertility Outcomes: A Review. Cureus. 2023;15(5):e38881.
[^5]: Hauser A, Levin I, Schwartz BI. The fallopian tube and its pathology: Paratubal cysts, tubal torsion, and pelvic inflammatory disease. Semin Pediatr Surg. 2025;37:151540.
[^6]: Tao X, Ge SQ, Chen L, Cai LS, Hwang MF, Wang CL. Relationships between female infertility and female genital infections and pelvic inflammatory disease: a population-based nested controlled study. Clinics (Sao Paulo). 2018;73:e364.
[^7]: Zuo Y, et al. Associations of Chlamydia trachomatis serology with fertility-related and pregnancy adverse outcomes in women: a systematic review and meta-analysis. eBioMedicine. 2023;94:104696.
[^8]: Li J, Li H, Liao J, Zhou L, Mo S, Zhang B, Lin Z, Shi Q, Chen Y. Tubal occlusion in patients with hydrosalpinx modifies the uterine environment and improves in vitro fertilization outcomes within 7 months. J Ovarian Res. 2025;18(1):223.
[^9]: Ou Y, Wang H, Zhou C, Chen Y, Lyu J, Feng M, Huang X. Endometriosis-associated infertility: Multi-omics insights into pathogenesis and precision therapeutics. Front Endocrinol. 2025;16:1613334.
[^10]: ASRM Practice Committee. Fertility evaluation of infertile women: a committee opinion. Fertil Steril. 2021;116(5):1255-1265.
[^11]: Briceag I, Costache A, Purcarea VL, et al. Current management of tubal infertility: from hysterosalpingography to ultrasonography and surgery. J Med Life. 2015;8(2):157-159.
[^12]: Mandia L, Personeni C, Antonazzo P, Angileri SA, Pinto A, Savasi V. Ultrasound in Infertility Setting: Optimal Strategy to Evaluate the Assessment of Tubal Patency. Biomed Res Int. 2017;2017:3205895.
[^13]: Ambildhuke K, Pajai S, Chimegave A, Mundhada R, Kabra P. A Review of Tubal Factors Affecting Fertility and its Management. Cureus. 2022;14(11):e30990.
[^14]: Kawwass JF, Crawford S, Kissin DM, Session DR, Boulet S, Jamieson DJ. Tubal factor infertility and perinatal risk after assisted reproductive technology. Obstet Gynecol. 2013;121(6):1263-1271.
[^15]: Trindade VD, Hentschke MR, Dornelles VC, et al. Tubal factor, cleavage stage and more than one embryo transferred were risk factors associated with ectopic pregnancy after assisted reproductive treatment. JBRA Assist Reprod. 2022;26(2):321-328.
[^16]: Vioreanu AM. The Psychological Impact of Infertility. Directions for the Development of Interventions. Mental Health: Global Challenges Journal. 2021;4(1).
[^17]: Sharma A, Shrivastava D. Psychological Problems Related to Infertility. Cureus. 2022;14(10):e30320.
This guide is for informational purposes only. Always consult qualified healthcare providers for personalized recommendations. For full details, read our Medical Disclaimer.

Author of the article
Date of publication


